Low-carb Diets (Risks When Ill), Vitamin C (Benefits When Ill)
The argument that carbs (or at least insulin, which you can get by eating a lot of protein also) help clear out degraded vitamin C is partially anecdotal, but seems reasonable to me:our last post, then it will substantially reduce oxalate excretion as well.Zero-carb dieters are at risk for
- Excess renal oxalate from failure to recycle vitamin C;
- Excess renal uric acid from disposal of nitrogen products of gluconeogenesis and ketogenesis;
- Salt and other electrolyte deficiencies from excretion of oxalate, urea and uric acid; and
- Dehydration.
These four conditions dramatically elevate the risk of kidney stones.
To remedy these deficiencies, we recommend that everyone who fasts or who follows a zero-carb diet obtain dietary and supplemental antioxidants, eat salt and other electrolytes, and drink lots of water.
Also, unless there is a therapeutic reason to restrict carbohydrates, it is best to obtain about 20% of calories from carbs in order to relieve the need to manufacture glucose and ketones from protein. This will substantially reduce uric acid excretion. If it also reduces vitamin C degradation rates, as we argued in
- An infection or some other stress (e.g. injury, cancer) leads to the oxidation of extracellular vitamin C; and
- On a low-insulin or glutathione-deficiency-inducing diet, oxidized vitamin C is not recycled.
The immune response to infections generates reactive oxygen species, which oxidize vitamin C. Oxidation removes a hydrogen atom from vitamin C, turning it into “dehydroascorbic acid,” or DHAA. If DHAA remains in the blood, it degrades with a half-life of 6 minutes. [3]
Infections can cause vitamin C deficiency on any diet. During the “acute phase response” to infection or injury, vitamin C often becomes deficient. Here is a nice paper in which French doctors surveyed their hospital patients for scurvy:
We determined serum ascorbic acid level (SAAL) and searched for clinical and biological signs of scurvy in 184 patients hospitalized during a 2-month period.
RESULTS: The prevalence of hypovitaminosis C (depletion: SAAL
So half were at least depleted in vitamin C and 17% had outright deficiency, which if it persisted would produce scurvy.
DHAA can be recycled back into vitamin C, but only inside cells.
DHAA transport is crucial for brain vitamin C status. There is no direct transport of vitamin C into the brain, yet the brain is one of the most vitamin C-dependent tissues in the body.
Supplying DHAA to stroke victims (of the mouse persuasion) as late as 3 hours after the stroke can reduce the stroke-damaged volume by up to 95%:
DHA (250 mg/kg or 500 mg/kg) administered at 3 h postischemia reduced infarct volume by 6- to 9-fold, to only 5% with the highest DHA dose (P
Once inside the cell, DHAA is recycled back to ascorbate, mainly by glutathione inside mitochondriaGlutathione is recycled mainly by an enzyme built with selenium. Zero-carb diets deplete selenium levels. Once that happens, you’ll have a Glutathione deficiency. (NAC is a Glutathione precursor, thus the recommendation to supplement if low-carb, especially if ill. You can also directly supplement Glutathione, taken with lots of water and no food). source: http://perfecthealthdiet.com/?p=1139 Vitamin C supplementation while ill makes sense, but you definitely want to have enough insulin and glutathione to recyle it to avoid the damage its “used” version creates:
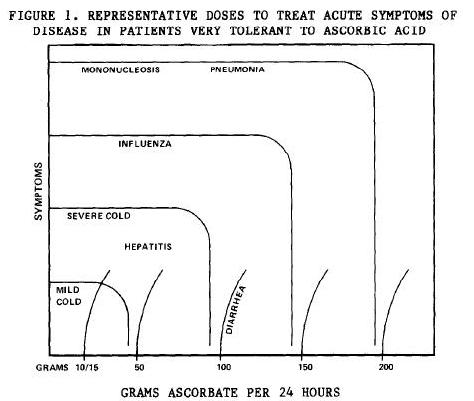
In 1970, I discovered that the sicker a patient was, the more ascorbic acid he would tolerate by mouth before diarrhea was produced. At least 80% of adult patients will tolerate 10 to 15 grams of ascorbic acid … The astonishing finding was that all patients … can take greater amounts of the substance orally without having diarrhea when ill or under stress. [5]
Extremely high dose intravenous vitamin C is effective in some cases.
The patient tries to TITRATE between that amount which begins to make him feel better and that amount which almost but not quite causes diarrhea. [5]
Recall that in animals, vitamin C synthesis rises as much as 100-fold under disease. In humans, the limit of bowel tolerance rises up to 20-fold during illness. This suggests that bowel tolerance limit is an indicator of need.Maybe. Bowel tolerance may be well over the optimum. But if it’s too hard to predict the optimum, it may be better than some fixed, modest amount.
it is my experience that ascorbate has little effect on the primary fungal infections
Nah. Maybe the 100g tolerated is quickly pissed/shit out. But say only 90% of it is wasted excess - then his point still carries weight. Speculation: it’s possible that Vit C is useful/protective against the poisonous ROS byproducts of the immune response, at a rate that exceeds the maximum recycling bandwidth via whatever (insulin+glutathione) is available. In that case, maybe the harm of the degraded Vit C is worth bearing.Well-nourished humans usually contain not much more than 5 grams of vitamin C in their bodies….
If a disease is toxic enough to allow for the person’s potential consumption of 100 grams of vitamin C, imagine what that disease must be doing to that possible 5 grams of ascorbate stored in the body. A condition of ACUTE INDUCED SCURVY is rapidly induced.
Conventional wisdom is correct in that only small amounts of vitamin C are necessary for this [antioxidant] function because of its [recycling and] repeated use. The point missed is that the limiting part in nonenzymatic free radical scavenging is the rate at which extra high-energy electrons are provided through NADH to re-reduce the vitamin C and other free radical scavengers. When ill, free radicals are formed at a rate faster than the high-energy electrons are made available. Doses of vitamin C as large as 1-10 g per 24 h do only limited good. However, when ascorbate is used in massive amounts, such as 30-200+ g per 24 h, these amounts directly provide the electrons necessary to quench the free radicals of almost any inflammation. Additionally, in high concentrations ascorbate reduces NAD(P)H and therefore can provide the high-energy electrons necessary to reduce the molecular oxygen used in the respiratory burst of phagocytes. In these functions, the ascorbate part is mostly wasted but the necessary high-energy electrons are provided in large amounts.I guess my speculation above is right.
Another early view was that vitamin C helps by destroying histamine, which may be produced in excess under conditions of stress.“early view”? sounds like it’s not a good view :)
the oxidized form of vitamin C, dehydroascorbate, has strong antiviral activity in vitro.DHAA is the (harmful) used vit-C byproduct that’s normally recycled.
in clinical experience, vitamin C is most effective against viral infections.
Since animals upregulate ascorbate production under all kinds of stress, not just viral infections, it seems probable that vitamin C aids health by multiple pathways, not only by antiviral activity.
Vitamin C is extremely safe. Intravenous doses of 120 g/day given to cancer patients have been well tolerated.
In animals such as chickens that lack the ability to synthesize vitamin C, vitamin C is recognized as a means of supporting bacterial and viral immunity.
A well-tested therapeutic strategy would be to take 4 g vitamin C every hour with water until bowel intolerance is reached. The therapy is extremely safe, and its effectiveness is usually apparent within days.
Supposedly low iodine and D are common with prolonged infections. Maybe selenium (may just be in case of low-carb). Meat has plenty of selenium, of course. Daily supplementation with high vit-C while not ill has some preliminary contraindicative research. Over-supplementing with vitamin E (fat soluble and toxic) is definitely bad. C might be ok.
(a) The Ristow paper administered vitamin E along with the C, see below for issues with that.
(b) Suppression of glutathione peroxidase and zinc-copper superoxide dismutase levels by C supplementation could be dependent upon levels of selenium and copper intake; so far only a small part of “supplement space” has been explored. What would be the effect of co-supplementation of C with selenium and copper?
(c) I can easily believe that vitamin C reduces the stress of exercise, but why isn’t the response to that more intense exercise, rather than elimination of vitamin C? Isn’t better tolerance of exercise a benefit for athletic training?
I’m not denigrating these papers, there could be reasons to avoid routine gram doses of C. But it needs more research. The benefits of C at 500 mg to 1 g/day in healthy people are more well established than these possible harms.
(2) The higher death rates are mainly in trials with vitamin E, sometimes beta carotene, both of which raise death rates on their own. When vitamin C is trialled on its own, the results have been mixed, but on my reading net positive.
In the case of C, our advice is more precautionary. Deficiency is tremendously harmful, but excess is virtually harmless. In trials, the benefit may be non-existent for 95%, but 5% may see big benefits and 0% harm. In trials the 95% dilute the benefits to the 5% out of statistical significance. Since the greatest benefit is likely to come in preventing infections from taking root, and everyone gets exposed to pathogens from time to time, we can’t know which of the 100% will benefit from the supplementation. So it makes sense to take a prophylactic supplement.
E and beta carotene seem to do damage. C and glutathione are essentially similar in status, C recycles glutathione and glutathione recycles C, so supplementing C is the most straightforward way to improve glutathione status. I happen to think glutathione is extremely beneficial and this is part of the reason I support C supplementation.
I do think you need a balance of the natural antioxidants, which is why copper and zinc (for zinc-copper superoxide dismutase) and selenium (for glutathione peroxidase) supplementation, and avoiding iron deficiency (for catalase), are important along with C supplementation.
We recommend obtaining vitamin E from foods only. If supplements are taken, they should supply low doses of mixed tocopherols and tocotrienols, not alpha-tocopherol only.
NAC we recommend for treating infections, not otherwise.(NAC is popular in bodybuilding supplements, most of which do nothing to grow muscle - the legal ones, at least)
C and selenium and a good diet, NAC in infections, should be sufficient to make liver glutathione.
Plant antioxidants I would avoid. I think the natural, mitochondrial antioxidants are going to be more beneficial than food antioxidants that don’t penetrate mitochondria (where antioxidants are most needed) and that suppress ROS signaling.weird. C is a plant antioxidant. carotenoids also (-> vit A) which give healthy (yellow-orange) looking skin and help immune function and neuron function. He must mean some other plant antioxidants (either tocopherols (vitamin-E like), polyphenolics (e.g. in balck tea, raspberries), or terpenoids (aromatic oils - citral, menthol, camphor, cannabinoids)?) source: http://perfecthealthdiet.com/?p=636